
BARCELONA, Spain - New data have shown a trend towards clinically meaningful improvements in survival and response rates and a favourable safety profile with first-line immunotherapy compared to current standard treatment for advanced hepatocellular carcinoma (HCC). (1)
The data, reported at the ESMO Congress 2019, despite not reaching its prespecified primary endpoint for improved overall survival, the CheckMate 459 study showed improvements in overall survival and response rates and a favourable safety profile in patients with advanced HCC treated with first-line nivolumab compared to sorafenib, a current standard of care.

“These results are important in the treatment of hepatocellular carcinoma, as there have been no significant advances over sorafenib in the first-line setting in more than a decade,” said study author Dr Thomas Yau, University of Hong Kong, China. He added: “HCC is often diagnosed in the advanced stage, where effective treatment options are limited. The encouraging efficacy and favourable safety profile seen with nivolumab demonstrates the potential benefit of immunotherapy as a first-line treatment for patients with this aggressive cancer.”
Yau acknowledged that the study did not meet the predefined threshold for statistically significant improvement in overall survival. “However, he said, “the primary analysis demonstrated a clinically meaningful overall survival benefit, which is particularly impactful considering the high frequency of subsequent use of systemic therapy, including immunotherapy in the sorafenib arm. Importantly, there was also a higher complete response rate with nivolumab compared to sorafenib.” He added that the patient-reported findings suggested that patients in the nivolumab arm experienced better quality of life and further supported clinical data that demonstrated a treatment benefit for nivolumab versus sorafenib in advanced HCC.
Commenting on the relevance of the new data, Dr Angela Lamarca, Christie NHS Foundation Trust, Manchester, UK, said, “In view of the fact that the CheckMate 459 study did not meet the predefined threshold of statistical significance for its primary end-point (overall survival), these results are unlikely to change the current standard of care. However, it is becoming more apparent that immunotherapy could have a role for the first-line treatment of advanced HCC and the differences in response rates are clinically meaningful.” She was disappointed that the higher response rate with nivolumab did not translate to improved progression-free survival or overall survival.
“The favourable safety profile with nivolumab is of relevance,” said Dr Lamarca. “The favourable safety profile becomes apparent in the form of less toxicity-related treatment discontinuation with nivolumab.” The potential impact on patients’ quality of life is also important, she added. “In a hypothetical scenario in which both options (sorafenib and immunotherapy) were available and reimbursed, and if quality of life was shown to be better with nivolumab (because of the better safety profile compared to sorafenib suggested in this study), clinicians and patients may favour the option with a more tolerable safety profile”. She concluded highlighting that this study did not meet its primary end-point and therefore conclusions were to be made cautiously and also that the high cost of immunotherapy could not be ignored.
Dr Lamarca noted that the well-designed study had two possible limitations, namely the unselected population and the predefined threshold of statistical significance. Results suggested patients with high PD-L1 had an increased response rate only in the nivolumab arm suggesting its potential role as a predictor biomarker; but she said, “More research is needed to better understand how to select patients for immunotherapy. PD-L1 looks promising in this study but we need a more reliable marker to select patients who will derive benefit.” “The lack of a reliable biomarker may have contributed to the study’s failure to show improved overall survival with immunotherapy”, she suggested. “In addition, the study design with a ‘high’ predefined threshold of statistical significance is generating confusion in the community with potentially beneficial therapies generating statistically negative studies”.
Study results
The phase 3 CheckMate 459 study randomised 743 patients with advanced hepatocellular carcinoma to nivolumab or sorafenib as first-line treatment.
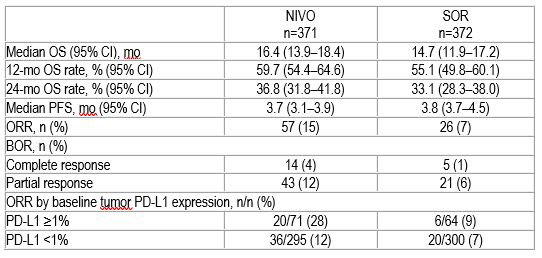
Median overall survival was 16.4 months for nivolumab and 14.7 months for sorafenib (hazard ratio [HR] 0.85; 95% confidence interval [CI]: 0.72-1.02; p=0.0752). This did not meet the predefined threshold of statistical significance. However, clinical benefit was observed across predefined subgroups of patients, including those with hepatitis infection and those with vascular invasion and/or extrahepatic spread.
The overall response rate was 15% for nivolumab (including 14 patients with complete response) and 7% for sorafenib (5 patients with complete response).
Grade 3 / 4 treatment-related adverse were reported in 22% of patients in the nivolumab arm (81 patients) and in 49% of those given sorafenib (179 patients). These led to discontinuation in 4% (16) and 8% (29) patients, respectively.
Official Congress Hashtag: #ESMO19
Social Media information
References
- LBA38_PR ‘Checkmate 459: A randomized, multi-center phase 3 study of nivolumab (nivo) vs sorafenib (sor) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (AHCC)’ will be presented by Thomas Yau during the proffered paper session on Friday, 27 September 2019, 14:00-15:30 CEST in Madrid Auditorium (Hall 2). Annals of Oncology, Volume 30, Supplement 5, October 2019
LBA38_PR - CheckMate 459: A Randomized, Multi-Center Phase 3 Study of Nivolumab (NIVO) vs Sorafenib (SOR) as First-Line (1L) Treatment in Patients (pts) With Advanced Hepatocellular Carcinoma (aHCC)
T. Yau1, J.W. Park2, R.S. Finn3, A.-L. Cheng4, P. Mathurin5, J. Edeline6, M. Kudo7, K.-H. Han8, J.J. Harding9, P. Merle10, O. Rosmorduc11, L. Wyrwicz12, E. Schott13, S.P. Choo14, R.K. Kelley15, D. Begic16, G. Chen17, J. Neely18, J. Anderson19, B. Sangro20
1Oncology, The University of Hong Kong, Pokfulam/Hong Kong PRC, 2Department Of Cancer Control And Population Health, Ncc-gcsp, Center for Liver Cancer, National Cancer Center, Goyang/Korea, Republic of, 3Medicine, Division Of Hematology And Oncology, David Geffen School of Medicine at UCLA, Los Angeles/United States of America, 4Medical Oncology, National Taiwan University Hospital Cancer Center, Taipei/Taiwan, 5Service D'hépatologie, Centre Hospitalo-Universitaire Claude Huriez, Lille/France, 6Arpego Network, Medical Oncology, Centre Eugene Marquis, Rennes/France, 7-, Kindai University Faculty of Medicine, Osaka/Japan, 8Internal Medicine, Severance Hospital, Yonsei University, Seoul/Korea, Republic of, 9Weill Medical College, Memorial Sloan-Kettering Cancer Center, New York/United States of America, 10Centre De Recherche En Cancérologie De Lyon, Hôpital de la Croix-Rousse, Lyon/France, 11Hepatogastroenterology, Assistance Publique Hôpitaux de Paris, Hôpital Pitié-Salpétrière – Université Pierre et Marie Curie, Paris/France, 12Department Of Gastrointestinal Cancer, M. Sklodowska-Curie Memorial Cancer Center and Institute of Oncology, Warsaw/Poland, 13Internal Medicine Ii - Gastroenterology, Hepatology And Diabetology, Helios Klinikum Emil von Behring GmbH, Klinik für Innere Medizin II, Berlin/Germany, 14Division Of Medical Oncology, National Cancer Centre Singapore, Singapore/Singapore, 15Medicine, University of California San Francisco, San Francisco/United States of America, 16Global Clinical Research/immuno-oncology, Bristol-Myers Squibb, Princeton/United States of America, 17Gbs - Oncology, Bristol-Myers Squibb, Princeton/United States of America, 18Immuno-oncology Biomarker Lead For Hcc & Scchn, Bristol-Myers Squibb, Princeton/United States of America, 19Immuno-oncology, Bristol-Myers Squibb, Princeton/United States of America, 20Liver Unit, Clinica Universidad de Navarra, Pamplona/Spain
Background: SOR is approved as 1L therapy for pts with aHCC, but there is still an unmet need to prolong survival and improve tolerability. This phase 3 study compared clinical efficacy and safety of NIVO with SOR as 1L therapy in pts with aHCC.
Methods: Systemic therapy–naive pts aged ≥18 years with aHCC were randomized 1:1 to NIVO (240 mg IV Q2W) or SOR (400 mg oral BID). Primary endpoint was overall survival (OS). Additional endpoints were objective response rate (ORR) and progression-free survival (PFS) by blinded independent central review per RECIST v1.1, efficacy by tumor programmed death ligand 1 (PD-L1) expression, and safety.
Results: 743 pts with aHCC were randomized to NIVO (n=371) or SOR (n=372) with minimum follow-up of 22.8 months at data cutoff. OS did not meet the predefined threshold of statistical significance (HR 0.84, P=0.0419). Median OS (mOS) was 16.4 mo for NIVO and 14.7 mo for SOR (HR 0.85 [95% CI: 0.72–1.02]; P=0.0752). Clinical benefit was observed across predefined subgroups, including hepatitis infection status, presence of vascular invasion and/or extrahepatic spread, and region (Asia vs non-Asia). ORR was 15% for NIVO (14 pts with complete response [CR]) and 7% for SOR (5 pts with CR; Table). Grade 3/4 treatment-related adverse events were reported in 81 pts (22%) in the NIVO arm and 179 pts (49%) in the SOR arm and led to discontinuation in 16 (4%) and 29 (8%) pts, respectively. No new safety signals were observed with NIVO. 140 pts (38%) in the NIVO arm and 170 pts (46%) in the SOR arm received subsequent therapy. Additional OS analyses and patient-reported outcomes will be presented to support the benefit of NIVO. Table: Efficacy results
Conclusions: Though the primary endpoint of OS did not achieve statistical significance vs SOR, NIVO showed clinically meaningful improvements in OS, ORR, and CR rate as 1L treatment for aHCC. NIVO demonstrated a favorable safety profile consistent with previous reports.
Clinical trial identification: NCT02576509
Editorial acknowledgement: Writing and editorial assistance was provided by Andrea L. Hammons of Parexel International (Waltham, MA, USA) and was funded by Bristol-Myers Squibb.
Legal entity responsible for the study: Bristol-Myers Squibb
Funding: Pharmaceutical, biotech, or other commercial company - Bristol-Myers Squibb
Disclosure: T. Yau: Honoraria (institution), Advisory / Consultancy: Bristol-Myers Squibb.
R.S. Finn: Honoraria (self), Speaker Bureau / Expert testimony: Astra Zeneca; Honoraria (self), Speaker Bureau / Expert testimony, Research grant / Funding (self): Bayer; Honoraria (self), Speaker Bureau / Expert testimony, Research grant / Funding (institution): Bristol-Myers Squibb; Honoraria (self), Speaker Bureau / Expert testimony, Research grant / Funding (institution): Eisai; Honoraria (self), Speaker Bureau / Expert testimony, Research grant / Funding (institution): Eli-Lilly; Honoraria (self), Speaker Bureau / Expert testimony, Research grant / Funding (institution): Merck; Honoraria (self), Speaker Bureau / Expert testimony: Novartis; Honoraria (self), Speaker Bureau / Expert testimony, Research grant / Funding (self): Pfizer; Honoraria (self), Speaker Bureau / Expert testimony: Roche/ Genentech.
A. Cheng: Honoraria (self), Advisory / Consultancy, Speaker Bureau / Expert testimony, Travel / Accommodation / Expenses: Ono Pharmaceutical; Advisory / Consultancy: Exelixis; Advisory / Consultancy: Nucleix Ltd.; Honoraria (self), Advisory / Consultancy, Travel / Accommodation / Expenses: Roche/Genentech; Honoraria (self), Advisory / Consultancy, Travel / Accommodation / Expenses: IQVIA; Advisory / Consultancy: Merck Sharp Dohme; Speaker Bureau / Expert testimony, Travel / Accommodation / Expenses: Bayer Yakuhin; Speaker Bureau / Expert testimony: Amgen Taiwan; Advisory / Consultancy: Ispen; Advisory / Consultancy: Bayer Schering Pharma; Advisory / Consultancy: Bristol-Myers Squibb; Honoraria (self), Advisory / Consultancy, Speaker Bureau / Expert testimony, Travel / Accommodation / Expenses: Eisai; Advisory / Consultancy: Merck Serono; Honoraria (institution), Advisory / Consultancy, Speaker Bureau / Expert testimony, Travel / Accommodation / Expenses: Novartis.
P. Mathurin: Honoraria (self), Speaker Bureau / Expert testimony: Ipsen; Honoraria (self), Speaker Bureau / Expert testimony: Eisai; Honoraria (self), Speaker Bureau / Expert testimony: MSD; Honoraria (self), Speaker Bureau / Expert testimony: Bayer Healthcare ; Honoraria (self), Speaker Bureau / Expert testimony: Abbvie; Honoraria (self), Speaker Bureau / Expert testimony: Gilead; Honoraria (self), Speaker Bureau / Expert testimony: Servier; Honoraria (self), Speaker Bureau / Expert testimony: Sanofi.
J. Edeline: Honoraria (self), Speaker Bureau / Expert testimony, Research grant / Funding (institution): Bristol-Myers Squibb; Honoraria (self), Speaker Bureau / Expert testimony: MSD; Honoraria (self), Speaker Bureau / Expert testimony: AstraZeneca; Honoraria (self), Speaker Bureau / Expert testimony: IPSEN; Honoraria (self), Speaker Bureau / Expert testimony: Eisai; Honoraria (self), Speaker Bureau / Expert testimony: Bayer; Travel / Accommodation / Expenses: AMGEN.
M. Kudo: Honoraria (self), Advisory / Consultancy, Speaker Bureau / Expert testimony: Bayer; Honoraria (self), Advisory / Consultancy, Speaker Bureau / Expert testimony, Research grant / Funding (institution): Eisai; Honoraria (self), Advisory / Consultancy, Speaker Bureau / Expert testimony: MSD; Advisory / Consultancy: Ono; Research grant / Funding (institution): Daiichi Sankyo; Research grant / Funding (institution): Medico's Hirata; Research grant / Funding (institution): Otsuka; Research grant / Funding (institution): Taiho; Research grant / Funding (institution): Astellas Pharma; Research grant / Funding (institution): Chugai; Research grant / Funding (institution): Bristol-Myers Squibb; Research grant / Funding (institution): EA Pharma; Research grant / Funding (institution): Takeda; Research grant / Funding (institution): Gilead.
J.J. Harding: Honoraria (self), Speaker Bureau / Expert testimony, Research grant / Funding (institution): Bristol-Myers Squibb; Honoraria (self), Speaker Bureau / Expert testimony: Eisai; Honoraria (self), Speaker Bureau / Expert testimony: Exelexis; Honoraria (self), Speaker Bureau / Expert testimony: Elly Lilly ; Honoraria (self), Speaker Bureau / Expert testimony: CytomX; Honoraria (self), Speaker Bureau / Expert testimony: QED.
P. Merle: Advisory / Consultancy: BAYER; Advisory / Consultancy, Research grant / Funding (institution): IPSEN; Advisory / Consultancy: EISAI; Advisory / Consultancy: LILLY; Advisory / Consultancy: Bristol-Myers Squibb; Advisory / Consultancy: MERCK; Speaker Bureau / Expert testimony: ROCHE; Advisory / Consultancy: ASTRA-ZENECA.
O. Rosmorduc: Honoraria (self): Bayer; Travel / Accommodation / Expenses: Bristol-Myers Squibb; Advisory / Consultancy: SIRTEX; Honoraria (self): EISAI.
L. Wyrwicz: Research grant / Funding (self): Bristol-Myers Squibb; Research grant / Funding (self): Beigene; Research grant / Funding (self): EISAI.
E. Schott: Honoraria (self): Bristol-Myers Squibb; Honoraria (self): Bayer.
S.P. Choo: Honoraria (self), Speaker Bureau / Expert testimony: Bayer; Honoraria (self), Speaker Bureau / Expert testimony: Lilly; Honoraria (self), Advisory / Consultancy, Speaker Bureau / Expert testimony: BMS; Honoraria (self), Advisory / Consultancy: Sirtex; Honoraria (self), Advisory / Consultancy: Eisai; Honoraria (self), Advisory / Consultancy: Ipsen.
R.K. Kelley: Advisory / Consultancy, Research grant / Funding (institution): Bristol Myers Squibb; Research grant / Funding (institution): Adaptimmune; Research grant / Funding (institution): Bayer; Research grant / Funding (institution): Eli Lilly; Research grant / Funding (institution): Exelixis; Honoraria (self), Speaker Bureau / Expert testimony, IDMC membership: Genentech/Roche; Research grant / Funding (institution): Merck; Research grant / Funding (institution): Regeneron; Research grant / Funding (institution): Astra Zeneca.
D. Begic: Full / Part-time employment: Bristol-Myers Squibb.
J. Neely: Shareholder / Stockholder / Stock options, Full / Part-time employment: Bristol-Myers Squibb.
J. Anderson: Shareholder / Stockholder / Stock options, Full / Part-time employment: Bristol-Myers Squibb.
B. Sangro: Advisory / Consultancy: Adaptimmune; Advisory / Consultancy: AstraZeneca; Advisory / Consultancy, Speaker Bureau / Expert testimony: Bayer; Advisory / Consultancy, Speaker Bureau / Expert testimony, Research grant / Funding (institution): Bristol-Myers Squibb; Advisory / Consultancy: BTG; Advisory / Consultancy: H3 Biomedicine; Advisory / Consultancy, Speaker Bureau / Expert testimony: Ipsen; Advisory / Consultancy: Lilly; Advisory / Consultancy: Merck; Advisory / Consultancy: Onxeo; Advisory / Consultancy, Speaker Bureau / Expert testimony, Research grant / Funding (institution): Sirtex Medical; Advisory / Consultancy: Roche; Advisory / Consultancy, Speaker Bureau / Expert testimony: TERUMO.
This press release contains information provided by the author of the highlighted abstract and reflects the content of this abstract. It does not necessarily reflect the views or opinions of ESMO who cannot be held responsible for the accuracy of the data. Commentators quoted in the press release are required to comply with the ESMO Declaration of Interests policy and the ESMO Code of Conduct.